Questions? Call us at 800-810-7790

A Pharmacist’s Guide to Heart Health
- Self reported statin intolerance ranges from 5–30%1
- Research shows the true prevalence is 9.1%
- Muscle pain is the #1 reason people stop taking statins
Meet Michael — He Struggled with Statin Side Effects And Found Zypitamag
After years of accepting muscle pain as "part of getting older," Michael talked to his doctor and learned about Zypitamag—a next-generation statin that is processed by the body differently.
He discovered that a 4mg dose of Zypitamag could deliver the same results as his old 40mg statin—with low rates of muscle pain and a "sugar-neutral" impact on his blood sugar levels. He’s now back to his active lifestyle thanks to a smarter approach to heart health.
Michael achieved the same cholesterol-lowering results as his previous high-dose statin without the discomfort that held him back.
High cholesterol is a major risk factor for heart disease. 1 out of every 4 cardiovascular deaths is connected to long term exposure to high LDL ("bad") cholesterol. For decades, statins have been the first line of defense. However, many people stop taking them due to side effects.
If you’ve struggled with statins, it’s important to know that "statin intolerance" isn't always permanent, and not all statins are created equal.
What is Statin Intolerance?
According to the National Lipid Association (NLA), statin intolerance occurs when a patient experiences adverse effects that improve when the dose is lowered or stopped.
To be clinically classified as "statin intolerant," a patient should generally have tried at least two different statins, including one at the lowest daily dose. It is categorized into two levels:
- Partial intolerance: You can handle a low dose, but not enough to reach your cholesterol goals.
- Complete intolerance: You cannot tolerate any dose of any statin.
Here’s what our pharmacist has to say about Statin Intolerance
How Common is It?
There is often a gap between "reported" side effects and what clinical trials show. A massive 2022 analysis of 176 studies involving over 4 million patients worldwide clarifies the stats:
- Self reported statin intolerance ranges from 5–30%
- Worldwide research shows the true prevalence is 9.1%
- Complete intolerance: Unable to tolerate any statin at any dose is less than 5%
The Nocebo Effect
Research suggests that some muscle pain is due to the "nocebo effect", where negative expectations lead to perceived side effects. These symptoms are still very real and need to be taken seriously.
While these feelings are real to the patient, they often mean the body can actually handle a statin if the right one is chosen.
Who is at Risk for Statin Intolerance?
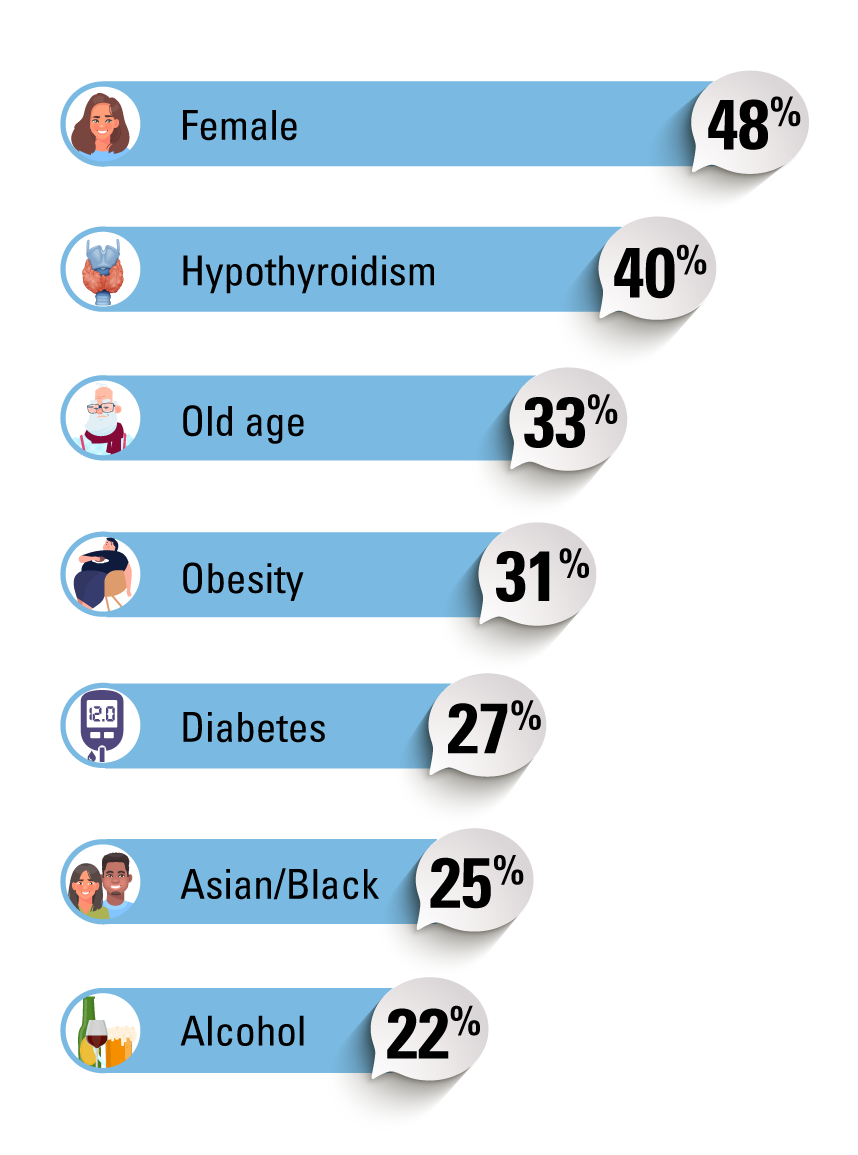
Factors associated with increased risk include:2:
- Female sex: 47.9% higher
- Older age, especially ≥ 65: 31% higher
- Asian: 25.4% higher or black race: 29.3% higher
- Obesity: 30.6% higher
- Hypothyroidism: 37.6% higher
- Diabetes: 26.6% higher
- Antiarrhythmics: 31.2% higher
- Alcohol use: 22% higher
- Intense exercise: 23.2% higher
- High statin dose: 37.5% higher
- Calcium channel blockers: 35.5% higher
- Chronic renal failure: 25.2% higher
- Chronic liver disease: 24.3% higher
Some factors that were not associated with a higher risk of statin intolerance included2:
- Smoking
- Arterial hypertension
- Duration of statin therapy
- White, Caucasian, or Hispanic race
- Warfarin
- Depression: 12.2% decreased risk
What Can You Do, If You Have Muscle Pain?
Many people regain tolerance by:
- Switching to a different statin
- Lowering the dose
- Using non daily dosing (e.g., every other day)
This step is important because not all statins are the same.
Not All Statins are the Same: Where Zypitamag Fits
There are 7 statins on the market. They differ in how they are processed in the body, how likely they are to interact with other drugs, and how often they cause muscle symptoms.
Zypitamag (pitavastatin) stands out in ways that matter for people worried about intolerance:
- Only 3.1% myalgia (muscle pain) rate
- Minimal CoQ10 depletion, which may reduce muscle pain.
- Lower risk of drug–drug interactions by using a less busy pathway
- Minimal impact on blood sugar
- 45% LDL-C reduction at 4 mg
Why This Matters
If someone has “failed” multiple statins, Zypitamag may still work because it behaves differently from other statins like atorvastatin or simvastatin.
Before giving up on statins entirely, try Zypitamag. It provides the powerful LDL‑lowering benefits of a statin but with one of the gentlest side‑effect profiles.
Zypitamag is an ideal option for those who:
- Have had issues with other statins
- Take multiple medications
- Need LDL-C lowering without high doses
- Are concerned about blood sugar increases
- Want well tolerated treatment backed by clinical evidence
Non Statin Options: How They Compare to Zypitamag
Zypitamag
- Mechanism: Blocks the liver’s main cholesterol-making enzyme (HMG‑CoA reductase).
- Efficacy: Lowers LDL-C by up to 45% and raises HDL-C by 8%.
- Cost: $39 or less for 30 days at Marley Drug
If Zypitamag is still not the right fit, or if you need extra help reaching your goals, several non-statin options exist.
Ezetimibe
- Mechanism: Works in the gut, blocking the small intestine from absorbing cholesterol from food and bile.
- Efficacy: Lowers LDL-C by 15–20% alone; 20–25% more when added to a statin.
- Cost: $37 for 180 days at Marley Drug
Nexletol (Bempedoic Acid)
- Mechanism: Blocks ACL, an enzyme the liver uses to make cholesterol. Works “upstream” of statins but becomes active mainly in the liver, not in muscle.
- Efficacy: Lowers LDL-C by 15-25% LDL-C alone; 15-17% more when added to statins; up to 35% with ezetimibe.
- Cost: $231 - $390/month
PCSK9 inhibitors (Repatha, Praluent, Inclisiran)
- Mechanism: Prevent destruction of LDL receptors in the liver, so the liver clears far more LDL from the blood. Given by injection.
- Efficacy: 50-60% LDL-C reduction alone.
- Cost: $240-$520/month
| Medication | LDL-C Reduction | Cost |
| Zypitamag: Blocks liver cholesterol production |
45% | $39/month or less at Marley Drug |
| Ezetimibe Blocks cholesterol absorption from the intestine |
15-20% | $37 for 6 months at Marley Drug |
| Nexletol: Blocks ACL enzyme in the liver (upstream from statins) |
15-25% | $231 - $390/month |
| PCSK9 Inhibitors (e.g., Repatha, Praluent, Inclisiran) Increase LDL receptor recycling so the liver removes more LDL |
Up to 60% | $240-$520/month |
Prices subject to change. This document is intended for educational purposes. We suggest bringing this information with you to discuss with your healthcare provider at your next visit.
The information on this page was informed by the following sources:
- Cheeley MK. et al. NLA scientific statement on statin intolerance: a new definition and key considerations for ASCVD risk reduction in the statin intolerant patient. Journal of Clinical Lipidology (2022) 16(4):P361-375. https://doi.org/10.1016/j.jacl.2022.05.068
- Bytyçi I. et al. Prevalence of statin intolerance: a meta-analysis. European Heart Journal (2022) 43(34):3213-3223. doi: 10.1093/eurheartj/ehac015
Related Topics

Compare Statins
Choosing the right statin for your lifestyle can be a daunting task. Use the guide below when discussing a statin therapy with your healthcare provider.

Ezetimibe (Zetia): For High Cholesterol
Ezetimibe (brand: Zetia) is a prescription medication used to lower high cholesterol. It is prescribed when a statin alone isn't doing enough, or for people who cannot tolerate high doses of statins. It can be taken by itself, but it is most often used as an "adjunct therapy" along with a statin.

How Statins Affect CoQ10 Levels and What That Means for You
Statins are among the most widely used medications globally, playing a crucial role in long-term health care. However, there's an interesting twist: statins can lower levels of Co-enzyme Q10 (CoQ10).

Repatha vs Statins
Repatha works by blocking a protein (PCSK9) that is responsible for destroying LDL receptors. By blocking this protein, Repatha allows more LDL receptors to remove excess cholesterol from the body.

9 Things You Should Know Before Taking Nexletol
Both Nexletol and statins work to lower the production of LDL-C (also known as "bad" cholesterol) in the liver, but they do so by targeting different enzymes. Statins work by blocking an enzyme called HMG-CoA reductase, while Nexleto

Praluent vs Statins
Praluent is usually recommended when statins or other cholesterol medication have not been successful at reaching your cholesterol goal.